Clinical directors operating within addiction treatment programs ohio face a consistent pressure point: balancing clinical quality with audit-ready compliance. In a partial hospitalization program ohio, that pressure intensifies due to higher payer scrutiny, documentation expectations, and staffing requirements.
If your goal is to reduce denials, protect revenue, and ensure regulatory alignment, your systems—not just your clinicians—must be built for consistency. Leveraging structured frameworks like those used in partial hospitalization program models can significantly improve both compliance outcomes and operational efficiency.
Documentation Systems That Withstand Payer Scrutiny
Documentation is the backbone of audit readiness—and the most common reason programs fail audits.
To meet compliance expectations, your PHP must consistently produce:
- Biopsychosocial assessments completed within defined timelines (typically 24–72 hours)
- Individualized treatment plans tied directly to DSM-based diagnoses and functional impairments
- Daily progress notes that reflect real interventions—not summaries
- Physician or qualified provider reviews at required intervals
The most frequent issue is generic documentation.
Payers are increasingly using AI-assisted audits to flag repetitive language patterns. If multiple notes contain identical phrasing, they are automatically flagged for review.
Operational Fix:
- Implement structured templates with required variation fields
- Require clinicians to document intervention + patient response + next step
- Conduct weekly documentation audits across a random sample (10–15% of charts)
Programs that shift from “completion-based documentation” to “defensibility-based documentation” see measurable reductions in audit risk.
Medical Necessity: The Revenue Gatekeeper
Every claim submitted for PHP services hinges on one question:
Why does this patient require this level of care today?
If your documentation cannot answer that clearly, reimbursement is at risk.
To establish medical necessity, documentation must show:
- Current symptoms and severity
- Functional impairment (social, occupational, behavioral)
- Risk factors (relapse, withdrawal, psychiatric instability)
- Failure or inappropriateness of lower levels of care
Example of weak documentation:
“Client continues to struggle with cravings.”
Audit-ready version:
“Client reports daily alcohol cravings rated 8/10, with two recent unsuccessful attempts to reduce use independently, indicating inability to maintain sobriety without structured intervention.”
That level of specificity directly correlates with:
- Authorization approvals
- Length of stay extensions
- Reduced payer pushback
Key Metric:
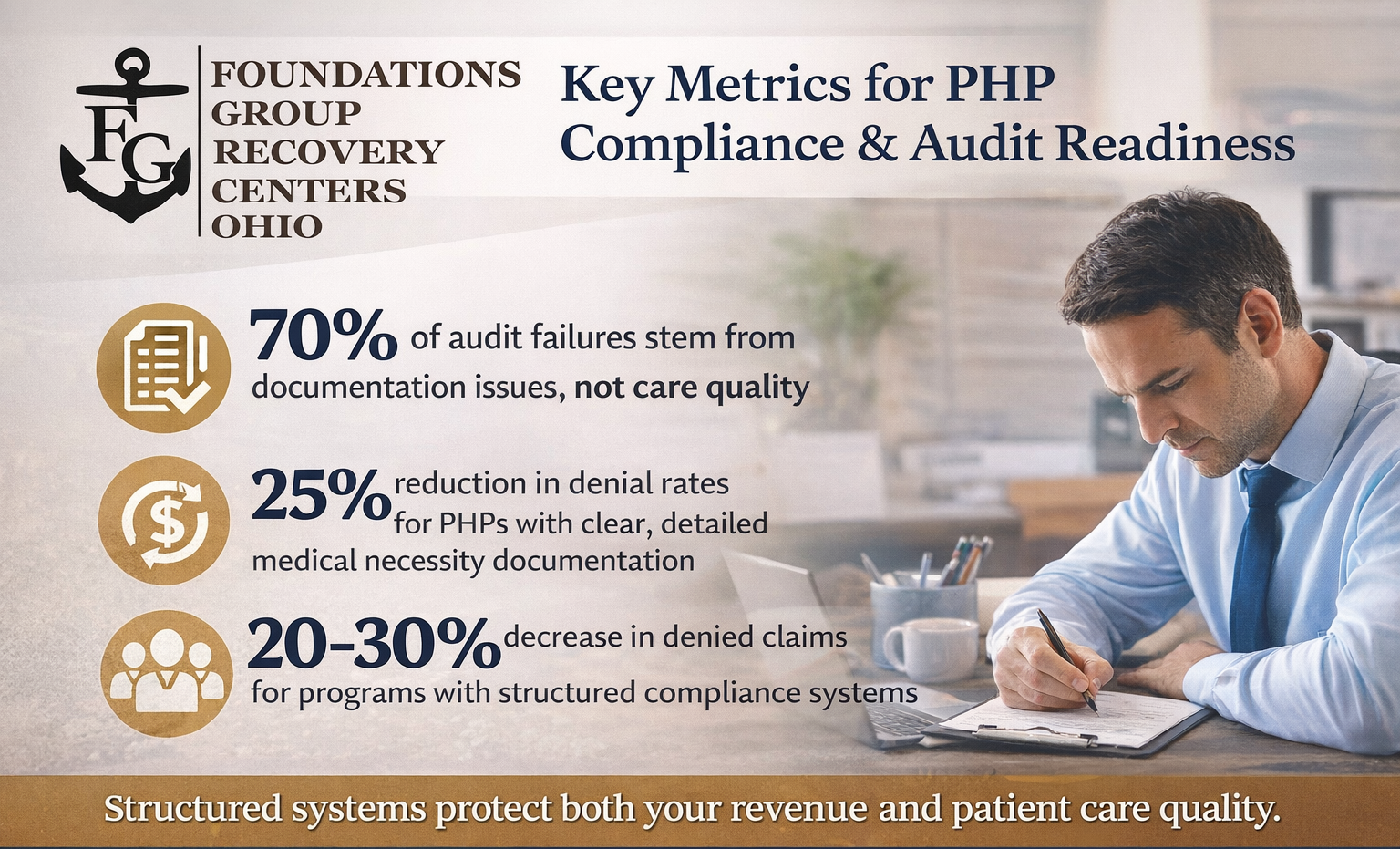
Programs with clearly documented medical necessity reduce denial rates by up to 25%.
Staffing Models That Meet Compliance and Clinical Demand
Meeting minimum staffing ratios is not enough. Compliance requires credential alignment, supervision structure, and real-time clinical availability.
A high-performing PHP staffing model includes:
- Licensed clinicians (LPC, LISW, LMFT) providing direct care
- Medical oversight (psychiatrist, physician, or nurse practitioner)
- Case managers coordinating continuity of care
- Clinical supervisors with documented oversight responsibilities
Where programs fail is in coverage gaps.
For example:
- No licensed clinician available during all programming hours
- Delayed physician reviews
- Lack of documented supervision
These gaps create both compliance risks and clinical inefficiencies.
Best Practice Framework:
- Maintain a staffing matrix by hour—not just by headcount
- Document supervision sessions weekly
- Align staff competencies with patient acuity levels
Structuring Daily Programming for Compliance and Outcomes
PHP is defined by intensity, structure, and clinical engagement.
Most payers expect:
- Minimum 20 hours of structured programming per week
- A blend of group therapy, individual therapy, and psychoeducation
- Evidence-based modalities such as CBT, DBT, and relapse prevention
But compliance depends on documentation quality—not just delivery.
Each session must reflect:
- Clinical objective tied to treatment plan
- Specific intervention used
- Patient engagement and response
Checklist for Directors:
- Are group notes individualized per patient?
- Are interventions clearly documented (not just topics)?
- Are outcomes measurable?
If the answer is no, your program is exposed—even if care quality is high.
Common Audit Failures and How to Prevent Them
Across payer audits, recurring issues include:
Cloned or Repetitive Notes
- Solution: Enforce narrative variation and audit language patterns
Missing Medical Necessity Justification
- Solution: Train staff to explicitly link symptoms to level of care
Outdated or Generic Treatment Plans
- Solution: Require updates every 7–14 days with measurable goals
Inconsistent Physician Documentation
- Solution: Schedule fixed review intervals and track completion
Attendance and Participation Gaps
- Solution: Implement real-time attendance tracking systems
Key Insight:
Over 70% of audit failures stem from documentation—not clinical care.
Building an Internal Compliance Framework
Sustainable compliance requires systemization.
A strong internal framework includes:
- Standardized documentation templates with mandatory fields
- Weekly internal audits with scoring systems
- Monthly compliance reporting dashboards
- Ongoing staff training based on audit findings
Recommended Audit Process:
- Randomly select 10–15% of active charts
- Score against predefined compliance criteria
- Identify patterns (not just individual errors)
- Implement corrective training within 7 days
Programs that adopt this approach shift from reactive compliance to proactive risk management.
Aligning Clinical Integrity With Financial Performance
Compliance is not just regulatory—it directly impacts revenue.
Strong systems lead to:
- Faster authorizations
- Higher approval rates for continued care
- Reduced claim denials
- Lower recoupment risk
Data Insight:
Programs with structured compliance systems report:
- 20–30% reduction in denied claims
- Improved average length of stay
- Stronger payer relationships
This is where clinical leadership drives business outcomes.
Local Operational Considerations That Impact Compliance
Programs operating in Franklin County, Ohio, particularly those serving patients in Columbus, Ohio, often face increased payer scrutiny due to higher service demand and network saturation.
This makes consistency even more critical.
Local success factors include:
- Strong documentation to differentiate from lower-performing providers
- Clear clinical pathways that justify level-of-care decisions
- Efficient staffing models that reduce burnout and turnover
In competitive regions, compliance is not just about avoiding penalties—it’s about maintaining payer trust and referral credibility.
Frequently Asked Questions for Clinical Directors
How often should PHP documentation be audited internally?
Weekly audits are recommended. Waiting for quarterly reviews increases risk exposure and delays corrective action.
What is the biggest compliance risk in PHP programs?
Lack of clear medical necessity documentation. Even strong clinical care can be denied without proper justification.
How detailed should progress notes be?
Notes should clearly document intervention, patient response, and next steps. Generic summaries are insufficient.
What staffing gaps create the highest risk?
Lack of licensed clinician availability during programming hours and inconsistent physician oversight are the most common issues.
How can programs reduce denial rates quickly?
Focus on improving documentation clarity, especially around medical necessity and treatment plan alignment.
Are templates helpful or harmful for compliance?
Templates are helpful only if they enforce specificity. Overuse without variation leads to audit flags.
Strengthen Your Program Before the Next Audit
If your PHP is scaling—or under increased scrutiny—now is the time to reinforce your systems.
Call (888)501-5618 to learn more about our Partial Hospitalization Program in Ohio.
Audit readiness isn’t built during an audit.
It’s built into your systems—every day.